
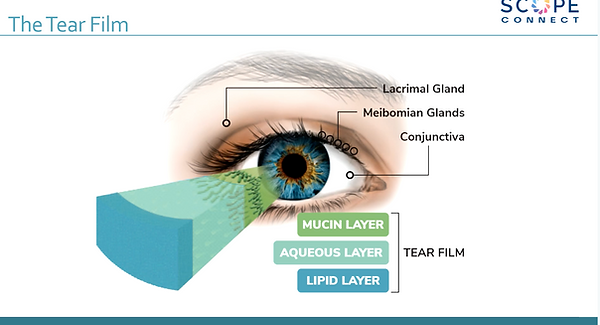
A Simplified view of the Tear Film
The tear film can be thought of as being made up of 3 layers. It is actually more complex than this. The deepest layer is the mucous layer that is secreted by the goblet cells on the conjunctiva. This layer spreads over the corneal surface and acts as the glue that holds the thickest layer, the watery or aqueous layer in place. The aqueous layer is prevented from evaporating and being lost by the lipid layer which is secreted by the meibomian glands that lie on the lid margin in a row behind the eyelashes. When we blink the muscles of the eyelids squeeze the meibomian gland to release their secretions and as the eyes reopen the aqueous and lipid layers are rasped over the ocular surface.
Recently our understanding of dry eye disease has improved in leaps and bounds and with it our realisation that IPL treatment can help many more dry eye variants than previously thought possible.
It was thought in the past that a patient had to be diagnosed as having either Aquous-Deficient Dry Eye or Evaporative Dry Eye and then tailoring their treatment to that exclusive diagnosis.
We now realise that the majority of dry eye, patients, about 86%,have a significant hyper-evaporative cause to their condition and only 10-14% have a purely aqueous secretion deficiency.
This means that treatments that help overcome causes of evaporative dry eye are very beneficial to the majority of dry eye patients.

A common component of both aqueous secretion deficiency and evaporative dry eye is that the tears residing on the ocular surface become over salty or hypertonic. The tears a patient secretes in cases of aqueous deficiency dry eye are over concentrated as they don't contain enough water ( Dart & Gilbard).
In evaporative dry eye it is only the water that is lost, also resulting in hypertonic over salty tears These abnormal tonicity tears cause inflammation throughout the ocular surface damaging the main and accessory aqueous secreting lacrimal glands and reducing the number of functional mucous secreting goblet cells. Gilbards impression cytology studies show the goblet cell drop-out as seen in this image comparing the normal healthy goblet cell density on the left with the reduced number present in a dry eye patient on the right -


This is why treatments such as IPL that stimulate the meibomian secretions to improve the lipid layer and reduce tear evaporation are so beneficial. IPL additionally reduces inflammation in the meibomian glands and ocular surface including the lacrimal glands. So a treatment originally thought to help with inflamed meibomian glands is actually helping all 3 layers of the tears.
In Sjogren's syndrome, primarily a severe form of aqueous deficient dry eye, these patients also often suffer from a much more severe form of meibomian gland inflammatory disease.
Not all Eyecare Practitioners appreciate this with their websites implying that only certain types of MGD benefit from IPL treatment, which is clearly misleading and not the case. (examples on file).